Gene Therapy for AADC: Targeting Neurons with AAV Vectors


Cell-specific delivery of genes is an attractive and desirable strategy for inherited rare diseases for its potential curative outcomes. Thus, adeno-associated virus (AAV) vectors have been increasingly used as delivery vehicles for developing gene therapies. Although AAVs have limited cargo capacity (i.e., < 5kb), their use in gene therapy reduces two significant concerns associated with other viral vectors, such as genomic integration and adverse immune reactions. Additionally, their specific tropism and transduction properties have already enabled successful treatment of various inherited conditions, including retinal diseases (e.g., Luxturna-AAV2), spinal muscular atrophy (e.g., Zolgensma-AAV9), and lipoprotein lipase deficiency (e.g., Glybera-AAV1, removed from the market due to limited use) (Domenger and Grimm, 2019).
Several gene therapies for rare CNS diseases (e.g., Giant Axonal Neuropathy-GAN, Angelman Syndrome, and Aromatic L-Amino Acid Decarboxylase Deficiency-AADC) are currently at different stages of preclinical and clinical evaluation that leverage AAV’s unique tropism to target neurons (Mendell et al. 2020). Among these, a recent report on the clinical success of an AAV2-based gene therapy for ADCC illustrates the continued growth and evolution of this approach.
What is AADC syndrome?
With only over 100 cases documented globally, AADC deficiency is a very rare autosomal recessive neurometabolic syndrome. Defects in AADC activity occur due to mutations in the DCC gene, which lead to deficits in the synthesis of the neurotransmitters serotonin and dopamine. Additionally, as dopamine is a precursor for synthesizing norepinephrine and epinephrine, AADC patients are also deficient in these neurotransmitters.
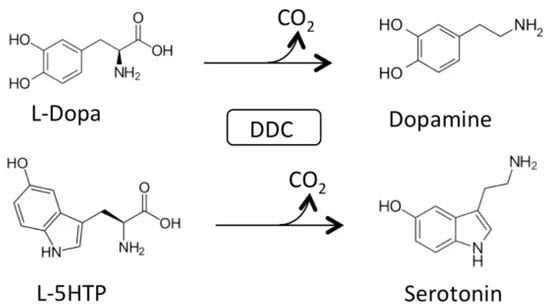
Main physiological reactions of Dopa decarboxylase (DDC). Decarboxylation of L-Dopa and L-5-HTP catalyzed by DDC. Retrieved from Montioli and Voltattorni, 2021 without modifications.
Individuals carrying DCC disease-causing mutations are afflicted from infancy. Phenotypes may vary from mild to very severe deficiencies in motor function and decreased muscle tone. Oculogyric crises, or involuntary eye movements typically upwards, are common in AADC patients (Solberg and Koht, 2017). Other common phenotypes include mood and sleep disorders.
Restoring AADC activity in the midbrain
In a new approach to the treatment of AADC deficiency, recently, investigators leveraged an AAV2 vector to target two midbrain regions, substantia nigra pars compacta (SNc) and ventral tegmental area (VTA), for delivery of the normal human AADC sequence (hAADC). Teams from Neurological Surgery Departments at the University of California San Francisco and Ohio State University designed the clinical study (ClinicalTrial NCT02852213) to evaluate the feasibility and safety of this new gene therapy strategy.
Previous clinical studies in Japan and Taiwan had targeted the putamen for AAV2-hAADC delivery (Hwu et al. 2012, Kojima et al. 2019). However, Pearson and colleagues believed that patients could achieve more significant benefits in improved motor function and behavioral and autonomic symptoms by restoring AADC activity and specifically dopamine biosynthesis in the SNc and VTA (Pearson et al. 2021).
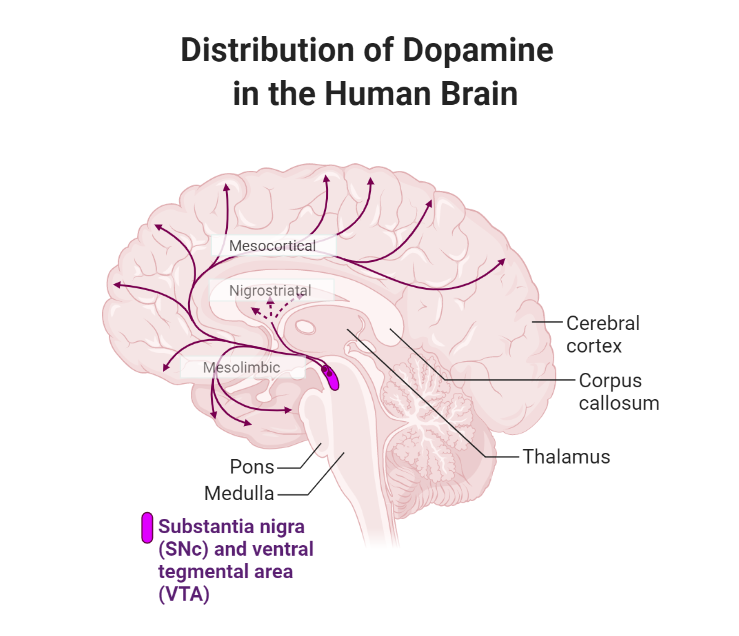
Distribution of dopamine in the human brain. Pearson and colleagues targeted the SNc and VTA with AAV2-hAADC to restore dopamine biosynthesis and neurotransmission in the nigrostriatal, mesolimbic, and mesocortical pathways. Adapted from “Distribution of Catecholamine Neurotransmitters in the Human Brain”, by BioRender.com (2021). Retrieved from https://app.biorender.com/biorender-templates
A total of seven pediatric patients with severe motor disabilities participated in the study and received magnetic resonance imaging-guided infusions of the AAV2-hAADC vector directly into the SNc and VTA. Pearson and colleagues confirmed successful AADC expression through increased tracer (FDOPA) uptake in targeted brain regions and dopamine metabolites in cerebrospinal fluid, which persisted after one and two years following gene therapy, respectively. Consistent with improved AADC activity, Oculogyric crises ended in most participants within a month after gene therapy. Motor functions such as head control and independent sitting were substantially improved one year after gene therapy in most participants. Significantly, two participants were able to perform supported walking a year after treatment. Lastly, AAV2-hAADC gene therapy improved behaviors such as mood, sleeping patterns, and feeding tolerance.
Overall, investigators found that AAV2-hAADC based gene therapy was safe and substantially contributed to improved quality of life for participants and their families. In addition, a significant advantage of this approach is the ability of AAV2-hAADC to transduce neurons in other brain regions through anterograde transneuronal transport, which investigators believe may have contributed to the positive outcomes of this study (Salegio et al. 2013).
Reference
Domenger, C. & Grimm, D. Next-generation AAV vectors-do not judge a virus (only) by its cover. Human Molecular Genetics (2019) doi:10.1093/hmg/ddz148.
Hwu, W. L. et al. Gene therapy for aromatic L-amino acid decarboxylase deficiency. Sci. Transl. Med. (2012) doi:10.1126/scitranslmed.3003640.
Kojima, K. et al. Gene therapy improves motor and mental function of aromatic l-amino acid decarboxylase deficiency. Brain (2019) doi:10.1093/brain/awy331.
Mendell, J. R. et al. Current Clinical Applications of In Vivo Gene Therapy with AAVs. Molecular Therapy (2021) doi:10.1016/j.ymthe.2020.12.007.
Montioli, R. & Voltattorni, C. B. Aromatic amino acid decarboxylase deficiency: The added value of biochemistry. International Journal of Molecular Sciences (2021) doi:10.3390/ijms22063146.
Pearson, T. S. et al. Gene therapy for aromatic L-amino acid decarboxylase deficiency by MR-guided direct delivery of AAV2-AADC to midbrain dopaminergic neurons. Nat. Commun. (2021) doi:10.1038/s41467-021-24524-8.
Salegio, E. A. et al. Axonal transport of adeno-associated viral vectors is serotype-dependent. Gene Ther. (2013) doi:10.1038/gt.2012.27.
Solberg, M. & Koht, J. Oculogyric crises. Tremor and Other Hyperkinetic Movements (2017) doi:10.7916/D85X2N2D.
- Like (2)
- Reply
-
Share




About Us · User Accounts and Benefits · Privacy Policy · Management Center · FAQs
© 2026 MolecularCloud