Advancing mRNA Medicines: Progressing Beyond Vaccines to Immunotherapies

The value of mRNA therapeutics has come into the general public’s attention by the rapid authorization and approval of high-efficacy mRNA vaccines (i.e., Moderna and Pfizer) for COVID-19. The seemingly whirlwind events leading to this new vaccine modality have created a combination of relief and apprehension, the latter particularly from those unaware of the long history of discoveries that have made possible today’s mRNA therapeutics. Nevertheless, the groundwork enabling the use of mRNA as drugs dates back to as early as the 1970s.
Progressing towards mRNA medicines
First, experiments in the 1970s by Lane et al., Stacey and Allfrey, and Maeyer-Guignard et al. showed the feasibility of transferring isolated mRNA into new cells (e.g., Xenopus oocytes, VERO cells, and HeLa cells) to achieve stable protein expression. While these studies relied primarily on mRNA microinjection, later work by Dimitriadis in 1978 leveraged liposomes to deliver intact and biologically active mRNA into mouse spleen lymphocytes. Next, in 1989, Malone et al. used lipofectin to transfect several cell types with in vitro transcribed mRNA. Later, the same group succeeded in driving the expression of synthetic mRNA in mouse skeletal muscle in vivo (Wolff et al. 1990). Ultimately, in 1993 and 1995, preclinical studies by Martinon et al. and Conry et al. were the first to evaluate immune responses to mRNA vaccines.
Many pioneering studies helped establish the feasibility of inducing protein expression through mRNA transfer into receptor systems. Nevertheless, barriers to successfully implementing mRNA as a therapeutic modality remained. For example, mRNA’s intrinsic instability, short persistence, and susceptibility to degradation limited protein production in vivo. Using in vitro-transcribed mRNA led to the activation of pro-inflammatory pathways, further reducing translation and promoting toxicity and cell death (Wadhwa et al. 2020, Xu et al. 2020, Ghattas et al. 2021). Therefore, modifications have been introduced to the basic mRNA structure to improve its stability, resistance to degradation by nucleases, translation efficiency, and modulate immunogenicity.
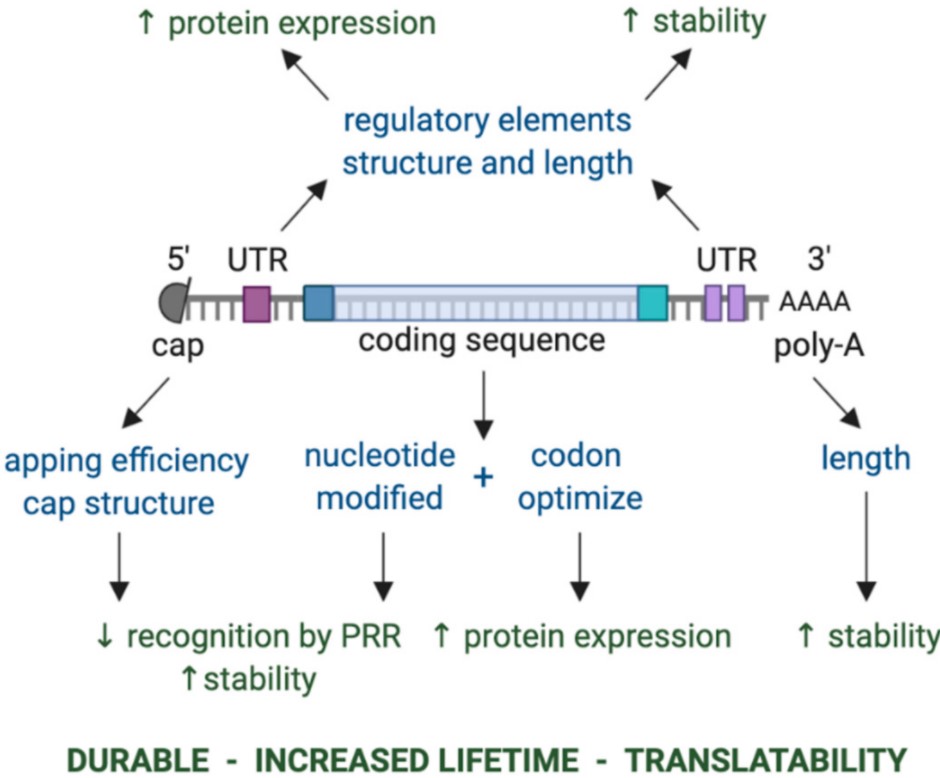
“Key components of in vitro transcribed mRNA that determine the level and duration of expression of the encoded protein. The components that can be modulated are shown in blue, while the effect of modulating these components is shown in green. Abbreviations: 3′ poly-A, three prime polyadenylic acid tail; 5′ cap, five prime cap; PRR, pattern recognition receptor; UTR, untranslated region.” Retrieved from Esprit et al. 2020, https://creativecommons.org/licenses/by/4.0/
For example, different cap analogs may be added to in vitro transcribed-mRNA to optimize its stability and translation and reduce immunogenicity (Wadhwa et al. 2020). Similarly, modified nucleosides have helped reduce innate immune stimulation through pattern recognition receptor activation (i.e., TLR 3, TLR7, and TLR8), ultimately improving protein expression (Kariko et al. 2004 and 2005). Furthermore, modulating the poly(A) tail’s length helps optimize mRNA stability and translation efficiency.
Beyond mRNA vaccines
COVID-19 mRNA vaccines are the culmination of significant progress over decades in developing strategies and platforms to support manufacturing mRNA therapeutics that are both efficacious and safe for clinical use. As a result, many more mRNA-based vaccines are in development. Currently, several candidates are in clinical studies for various infectious diseases, such as Influenza, Zika, Chikungunya, and HIV. In addition, some vaccine candidates have progressed to Phase III clinical studies, including mRNA-1345 (Respiratory Syncytial Virus) and mRNA-1647 (Cytomegalovirus).
As a therapeutic modality, mRNA has the potential of providing curative solutions for a host of disease states through different mechanisms. Beyond vaccine modalities for infectious diseases, mRNA is valuable as a mechanism to develop immunotherapies for cancer. As such, mRNA cancer vaccines are being developed and studied for a broad range of solid tumors (e.g., melanoma-BNT111, glioblastoma-RNA-LP, and colorectal neoplasms-mRNA-5671/V941). Clinical studies are also underway for mRNA therapeutics encoding antibodies (BNT141/142) and cytokines (BNT152/153) for solid tumors. Additionally, mRNA-based cell immunotherapeutics, such as autologous mRNA-CAR or TCR T celltherapies, provide means to temporarily target tumor antigens, which may reduce adverse events (e.g., cytokine release syndrome) associated with using genetically engineered T cells (Van Hoecke et al. 2021).
More recently, preclinical studies at the University of Pennsylvania Perelman School of Medicine, led by Dr. Jonathan Epstein, are extending the use of mRNA-CAR T cell immunotherapies to provide an innovative solution to a different aliment, cardiac fibrosis (Rurik et al. 2022). Myocardial infarction is the most common cause of fibrotic scarring of the cardiac muscle. In cardiac fibrosis, pathological changes in the extracellular matrix brought about by increased collagen type I deposition and cardiac fibroblast activation affect the heart’s muscle function (Hinderer and Schenke-Layland, 2019).
Previous findings by Dr. Epstein’s team demonstrated that targeting activated fibroblasts with CD8+ cytotoxic CAR T cells ameliorated cardiac fibrosis and restored function in a mouse model of cardiac injury (Aghajanian et al. 2019). Nevertheless, while effective, such approach could indefinitely impact the process of fibrosis. Therefore, Epstein’s team opted for a more conservative strategy that would only transiently target activated fibroblast. To achieve this, the team designed an mRNA-CAR against activated fibroblasts (anti-Fibroblast Activated Protein or FAPCAR), which they encapsulated into lipid nanoparticles decorated with antibodies to CD5 (CD5/LNPs). In vivo administration of this new mRNA therapeutic effectively transfected T cells (CD4+>CD8+) and resulted in functional anti-FAP CAR T cells. Moreover, in a mouse model of cardiac injury, CD5/LNP-FAPCAR mRNA administration led to improved cardiac function and reduced fibrosis.
Overall, significant obstacles have been cleared by the innovation and tenacity of many scientists over decades, making the use of mRNA therapeutics a reality. Delivery limitations remain, especially for large molecules, systemic administration, and targeting specific tissues. Nevertheless, mRNA therapeutics provide new options for many diseases, including rare and not so rare disease states.
How much do you know about mRNA Therapeutics?
Take the Quiz, test your mRNA knowledge, and try your luck at some cool prizes.
- Like (5)
- Reply
-
Share




About Us · User Accounts and Benefits · Privacy Policy · Management Center · FAQs
© 2026 MolecularCloud